The Winter Breakthrough
Clinical Vignette
A 46-year-old woman with acute myeloid leukemia is admitted on day 83 after matched unrelated donor allogeneic hematopoietic stem cell transplantation. Her post-transplant course has been complicated by grade II gastrointestinal graft-versus-host disease treated with tacrolimus and prednisone 20 mg daily. She is receiving trimethoprim-sulfamethoxazole, acyclovir, and letermovir prophylaxis. Four days before presentation, her 7-year-old granddaughter visited while febrile with cough and rhinorrhea.
She now reports two days of fever, diffuse myalgias, sore throat, dry cough, and rapidly progressive dyspnea. On arrival, temperature is 38.7 C, heart rate 118/min, blood pressure 108/64 mmHg, respiratory rate 26/min, and oxygen saturation 89% on room air, improving to 95% with 4 L/min nasal cannula. She appears ill and fatigued. Lung examination reveals diffuse inspiratory crackles without wheezing. There is no rash, meningismus, or lower extremity edema.
Laboratory studies show white blood cells 2.1 x 10^3/uL with an absolute lymphocyte count of 0.3 x 10^3/uL, hemoglobin 9.4 g/dL, platelets 74 x 10^3/uL, creatinine 1.0 mg/dL, AST 68 U/L, ALT 54 U/L, and procalcitonin 0.16 ng/mL. Nasopharyngeal multiplex polymerase chain reaction testing is positive for influenza A and negative for SARS-CoV-2, RSV, and adenovirus. Chest radiograph demonstrates new patchy bilateral perihilar and bibasilar airspace opacities.
Oseltamivir is started and she is placed on droplet precautions. During rounds, the fellow is asked to explain how influenza establishes infection in the respiratory tract, why oseltamivir works, and why prevention still depends on annual vaccination and protection of close contacts even in previously vaccinated households.
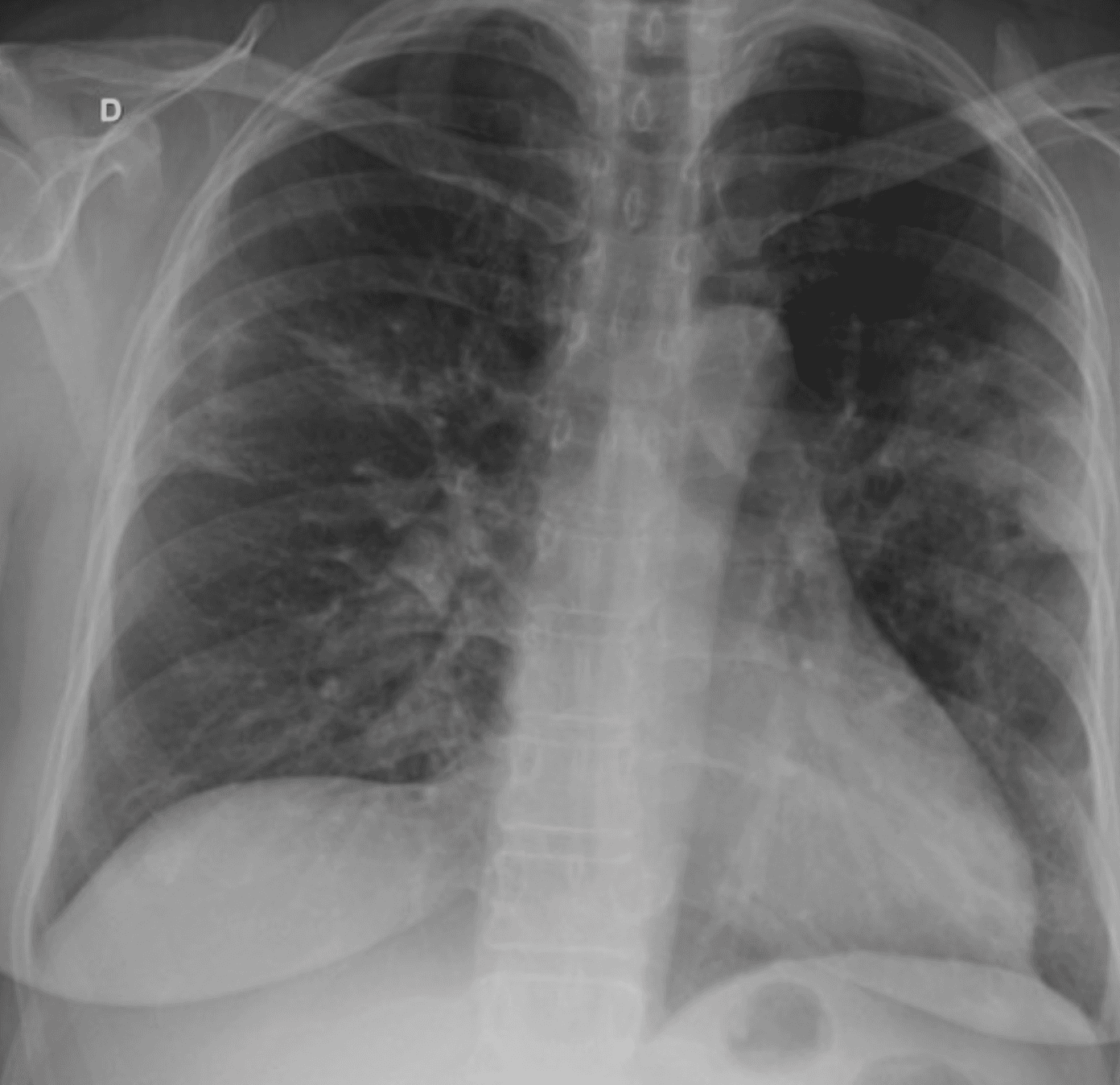
Chest radiograph demonstrating bilateral patchy airspace opacities consistent with viral pneumonia.
Question 1
Which viral mechanism best explains how influenza A initially establishes infection in the respiratory epithelium?
Select one option to submit your answer and view live poll results.
Question 2
Which statement best explains why oseltamivir is active against this infection?
Select one option to submit your answer and view live poll results.
Question 3
Which virologic mechanism most directly explains why influenza prevention still requires updated annual vaccination for this patient's household contacts and healthcare workers?
Select one option to submit your answer and view live poll results.
References
Krammer F, Smith GJD, Fouchier RAM, et al. Influenza. Nat Rev Dis Primers. 2018;4(1):3.
Taubenberger JK, Morens DM. The pathology of influenza virus infections. Annu Rev Pathol. 2008;3:499-522.
Uyeki TM, Bernstein HH, Bradley JS, et al. Clinical practice guidelines by the Infectious Diseases Society of America: 2018 update on diagnosis, treatment, chemoprophylaxis, and institutional outbreak management of seasonal influenza. Clin Infect Dis. 2019;68(6):e1-e47.
Hayden FG, Sugaya N, Hirotsu N, et al. Baloxavir marboxil for uncomplicated influenza in adults and adolescents. N Engl J Med. 2018;379(10):913-923.