Memory Lost
Clinical Vignette
A 51-year-old man with acute myeloid leukemia presents on day 38 following allogeneic hematopoietic stem cell transplantation from a matched unrelated donor. He received myeloablative conditioning with busulfan and cyclophosphamide and has developed grade II chronic graft-versus-host disease affecting the skin and liver, managed with tacrolimus 2 mg twice daily and mycophenolate mofetil 1 g twice daily. Pretransplant serologies were notable for HSV IgG negative and VZV IgG negative; accordingly, acyclovir prophylaxis was not initiated. He is on fluconazole, trimethoprim-sulfamethoxazole, and letermovir for CMV prophylaxis (donor CMV seropositive, recipient seronegative).
Over the past five days his family has noted progressive confusion and short-term memory loss: he cannot recall conversations from an hour earlier, repeatedly asks the same questions, and has become increasingly disoriented to time. This morning he had a witnessed generalized tonic-clonic seizure lasting 90 seconds, which resolved spontaneously. He has had no fever, no headache, and no focal neurologic deficits. His wife notes he has seemed "not himself" for about a week.
On examination he is afebrile, blood pressure 128/74 mmHg, heart rate 88 bpm. He is alert but disoriented to date and place. He cannot recall three words after five minutes. There is no papilledema, no meningismus, and no focal motor or sensory deficits. Serum sodium is 126 mEq/L with urine osmolality 480 mOsm/kg and urine sodium 48 mEq/L, consistent with the syndrome of inappropriate antidiuretic hormone secretion. Serum CMV PCR is undetectable. EEG shows diffuse slowing with left temporal sharp waves.
MRI of the brain with and without gadolinium is performed.
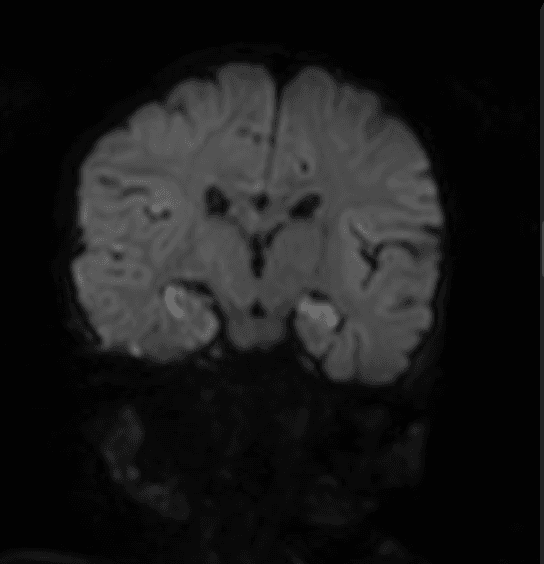
MRI brain, FLAIR sequence: bilateral T2/FLAIR hyperintensity involving the mesial temporal lobes, hippocampi, and amygdalae, without significant gadolinium enhancement. Pattern consistent with limbic encephalitis.
Question 1
Which of the following is the most likely cause of this patient's limbic encephalitis?
Select one option to submit your answer and view live poll results.
Question 2
The team sends both a serum HHV-6 PCR and a CSF HHV-6 PCR as part of the workup. The serum HHV-6 PCR returns at an extraordinarily high level: greater than 10 million copies/mL. Before the CSF result is available, what is the most important consideration regarding the serum result?
Select one option to submit your answer and view live poll results.
Question 3
CSF HHV-6 PCR returns positive at 48,000 copies/mL. HSV, VZV, CMV, and EBV PCRs are all negative. The diagnosis of HHV-6 encephalitis is confirmed. What is the treatment of choice?
Select one option to submit your answer and view live poll results.
References
Zerr DM, Gupta D, Huang ML, Carter R, Corey L. Effect of antivirals on human herpesvirus 6 replication in hematopoietic stem cell transplant recipients. Clinical Infectious Diseases. 2002;34(3):309-317.
Bhatt N, et al. A contemporary review of HHV-6 encephalitis in allogeneic hematopoietic cell transplant recipients: what every transplant infectious disease clinician should know. Transplant Infectious Disease. 2021;23(1):e13430.
Pellett PE, et al. Chromosomally integrated human herpesvirus 6: questions and answers. Reviews in Medical Virology. 2012;22(3):144-155.
Hill JA, et al. Outcomes of HHV-6 encephalitis in allogeneic hematopoietic cell transplant recipients: a multicenter study. Clinical Infectious Diseases. 2021;72(9):1527-1535.