Forgotten but Not Gone
Clinical Vignette
A 38-year-old man with alcohol use disorder is brought to the emergency department by his roommate after being found confused and difficult to arouse. His roommate reports he had complained of headache and neck stiffness for two days and had been febrile and vomiting since the previous evening. He has no significant medical history and takes no medications. His vaccination records are unavailable.
On examination he is febrile to 39.9°C, blood pressure 98/62 mmHg, heart rate 118 bpm, and respiratory rate 22 breaths per minute. He is somnolent and oriented only to person. There is severe nuchal rigidity and a positive Kernig sign. No petechiae or purpuric lesions are identified. Fundoscopic examination shows no papilledema. CT of the head without contrast is obtained urgently and shows no mass lesion or midline shift.
Lumbar puncture is performed immediately. Opening pressure is 38 cmH₂O. CSF appears frankly turbid. CSF white cell count is 4,200/μL with 94% neutrophils; protein is 318 mg/dL; glucose is 18 mg/dL with simultaneous serum glucose of 104 mg/dL. Two sets of blood cultures are drawn and empiric therapy with vancomycin, ceftriaxone, ampicillin, and dexamethasone is initiated immediately. The CSF Gram stain result revealed:
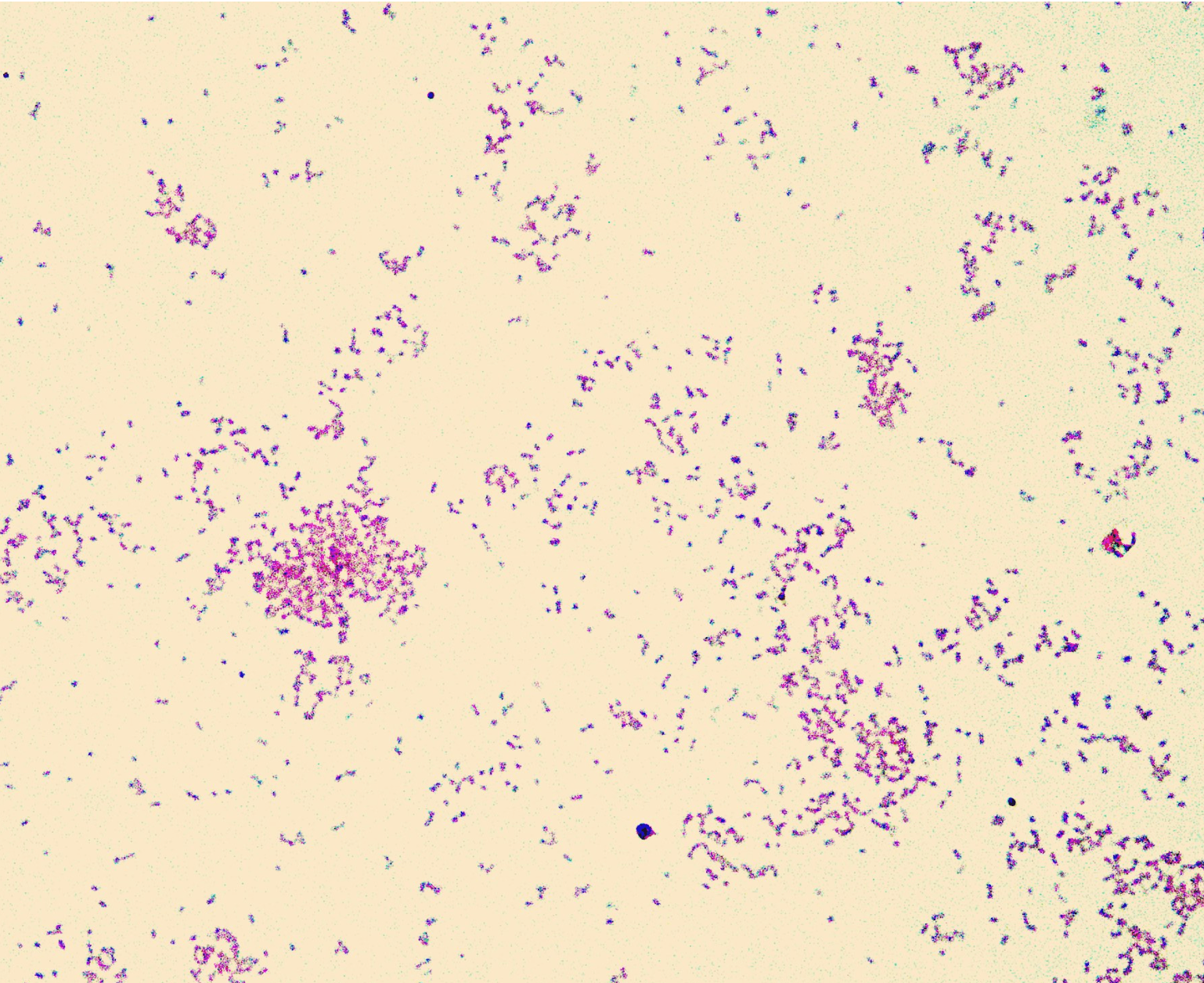
CSF Gram stain: small, pleomorphic gram-negative coccobacilli, seen singly and in pairs. The organisms range from coccoid to short rod forms.
Image source: PathologyOutlines.com
Question 1
Which organism is most consistent with this morphology and clinical presentation?
Select one option to submit your answer and view live poll results.
Question 2
What is the most appropriate antibiotic management at this point?
Select one option to submit your answer and view live poll results.
Question 3
The patient has a roommate and two household contacts who spent significant time with him in the week before admission. What is the appropriate management for close contacts?
Select one option to submit your answer and view live poll results.
References
van de Beek D, de Gans J, Tunkel AR, Wijdicks EF. Community-acquired bacterial meningitis in adults. New England Journal of Medicine. 2006;354(1):44-53.
de Gans J, van de Beek D; European Dexamethasone in Adulthood Bacterial Meningitis Study Investigators. Dexamethasone in adults with bacterial meningitis. New England Journal of Medicine. 2002;347(20):1549-1556.
Centers for Disease Control and Prevention. Haemophilus influenzae type b: prevention and control of Hib disease. MMWR Recommendations and Reports. 2014.
Tunkel AR, et al. Practice guidelines for the management of bacterial meningitis. Clinical Infectious Diseases. 2004;39(9):1267-1284.