The Loyal Companion
Clinical Vignette
A 58-year-old woman is brought to the emergency department by her husband after he found her confused and febrile at home. Over the preceding three days she had developed worsening fever, chills, and fatigue; on the morning of presentation she was difficult to rouse. Her medical history is notable for a splenectomy performed 15 years earlier following a motor vehicle accident, and rheumatoid arthritis managed with low-dose prednisone 5 mg daily for the past four years. She received her pneumococcal, meningococcal, and Haemophilus influenzae type b vaccines at the time of splenectomy but has not had booster doses. She does not use alcohol or tobacco and takes no other medications.
On review of systems her husband reports she has not been bitten by any animal and has not traveled recently. She has a golden retriever that sleeps in the bedroom; the dog frequently licks her hands and forearms. She has mild eczema affecting both forearms with areas of excoriated, non-intact skin.
On examination she is febrile to 39.8°C, blood pressure 82/50 mmHg, heart rate 122 bpm, and respiratory rate 26 breaths per minute. She is somnolent and oriented only to person. There is no nuchal rigidity on initial assessment; no skin rash or petechiae are identified. The remainder of the examination is unremarkable.
White blood cell count is 18,400/μL with 88% neutrophils and 14 bands. Platelet count is 54,000/μL. INR is 1.8. Serum lactate is 4.2 mmol/L. Creatinine is 1.9 mg/dL. Lumbar puncture is performed after CT of the head: opening pressure 28 cmH₂O; CSF white cell count 2,400/μL with 94% neutrophils; CSF protein 292 mg/dL; CSF glucose 26 mg/dL with serum glucose 110 mg/dL. Empiric therapy with vancomycin, ceftriaxone, ampicillin, and dexamethasone is started. Two sets of blood cultures are drawn prior to antibiotics.
At 72 hours, one blood culture bottle flags positive. The Gram stain shows slender, elongated, fusiform gram-negative rods with tapered ends arranged singly and in loose aggregates. The laboratory notes the organism is fastidious, required CO₂-enriched conditions to grow, and failed to grow on MacConkey agar.
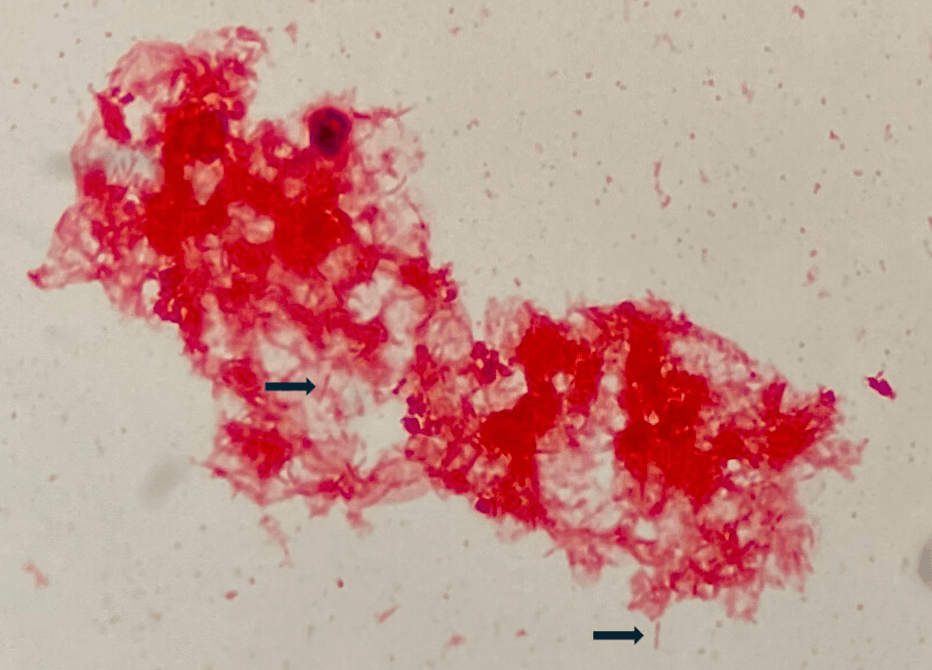
Gram stain from blood culture: slender, elongated, fusiform gram-negative rods with tapered ends. Image from Sooter et al., ASM Case Reports, 2024 (DOI: 10.1128/asmcr.00085-24).
Question 1
Which of the following organisms is most consistent with this blood culture morphology and clinical presentation?
Select one option to submit your answer and view live poll results.
Question 2
Susceptibility testing returns: susceptible to ampicillin-sulbactam, meropenem, and clindamycin; resistant to aztreonam. What is the most appropriate next treatment?
Select one option to submit your answer and view live poll results.
References
Westwell AJ, Kerr KG, Spencer MB, Hutchinson DN. Capnocytophaga canimorsus septicaemia in an asplenic patient. Journal of Infection. 1989;18(2):165-167.
Pers C, Gahrn-Hansen B, Frederiksen W. Capnocytophaga canimorsus septicemia in Denmark, 1982-1995: review of 39 cases. Clinical Infectious Diseases. 1996;23(1):71-75.
Lion C, Escande F, Burdin JC. Capnocytophaga canimorsus infections in human: review of the literature and case report. European Journal of Epidemiology. 1996;12(5):521-533.
Sooter AJ, et al. Capnocytophaga canimorsus meningitis in an immunocompromised host. ASM Case Reports. 2024.